 This is my second response to Associate Professor Rita Barnett-Rose to her paper “Compulsory water fluoridation: justifiable public health benefit or human experimental research without informed consent”.
This is my second response to Associate Professor Rita Barnett-Rose to her paper “Compulsory water fluoridation: justifiable public health benefit or human experimental research without informed consent”.
Again I wish to thank Rita for acknowledging in that papers should be referenced accurately by using citations to the original sources rather than simply referring to activist sources. I am also pleased she is getting experts to review the science in her paper and am interested to know who the independent reviewers are.
My response looks into fluoridation on objectively looking at the science, what the evidence shows, ethics and The World Health Organization.
Rita’s original paper here. My first response here. Rita’s first response here.
You can read the PDF version here.
Compulsory Water Fluoridation: Second Response To Rita Barnett-rose
Written by Daniel Ryan
Introduction
This is my second response to Associate Professor Rita Barnett-Rose to her paper “Compulsory water fluoridation: justifiable public health benefit or human experimental research without informed consent”. It is a response to her document “RE: CWF Working Paper Article” (hereafter referred to as “Rita’s reply.”). I wish to thank Rita for acknowledging in that papers should be referenced accurately by using citations to the original sources rather than simply referencing activist sources. I am also pleased she is getting experts to review the science in her paper and am interested to know who the independent reviewers are.
In this response I have collected a number of comments to consider under separate headings.
Objectively looking at the science.
Rita’s reply:
“…you object to my failure to include contrary studies that reaffirm the (English speaking countries’) public health agencies’/dental lobby positions on the safety and benefits of compulsory water fluoridation.”
“…with respect to your complaint or desire that I cite to contrary (i.e., pro-fluoridation) studies in addition to (or in lieu of) the published studies that I cite that tend to weigh against fluoridation”
“It is not meant to be an exhaustive examination of all studies on fluoridation and is specifically and accurately identified for what it is”
“…you are just as guilty of ‘cherry picking’ your sources and your studies as you suggest I am.”
“I am not interested in a battle of the studies debate”
“These reasons would remain even if compulsory water fluoridation were proven to be entirely safe, which it most definitely has not, despite the presumed “majority” view in the English speaking countries”
My reply:
Rita implies I only use ‘pro-fluoridation’ or ‘English speaking countries’ papers. This is incorrect – I cite papers which provide the best weight in regards to evidence. Science doesn’t take sides (good papers are neither “anti-fluoridation” nor “pro-fluoridation”, they present data and reasoning) and these are international. To clarify, my issue is not that Barnett-Rose (2014) was not using ‘pro-fluoridation’ papers, it was the quality of the studies themselves. Reviewers of the science should attempt to understand and evaluate the quality of the research.
I also look at the quality of journal. And I try to cite papers which are in high quality journals more as those journals attract the best scientific papers. Journals use a metric called “impact factor” that basically states how many times an average paper is cited by other papers. It is an independent, objective method to judge the quality of published research.
The hierarchy of scientific evidence in the literature is also important I illustrate this in the image below.

Secondary reviews published in peer-reviewed, high-impact journals and high quality randomised controlled trials with definitive results should be the preferred sources. For consideration of human health effects I consider that animal studies would be placed above “expert opinion” in this hierarchy.
Overall one needs to approach the literature intelligently and critically – considering the evidence provided in the individual papers and also considering other published material.
Instead I saw that Barnett-Rose (2014) did not evaluate the evidence well, only selecting evidence of harm in order to persuade the audience to accept her position. There is no reason to use low validity papers when there is plenty of high quality papers but unfortunately this happens when trying to “price” a preconceived idea.
An example of this is Barnett-Rose (2014) used an opinion article from the Scientific American many times as her source. This is not a scientific paper, it is not peer-reviewed or in a research journal; furthermore the writer is not a scientist and definitely not an expert on the subject. This type of evidence would come below “expert opinion” on the image above. I hope such problems would be given as feedback from the independent reviewers.
Rita accuses me of cherry picking but fails to back this up. I do try to use only the best sources of evidence – usually systematic reviews. A systematic review is a literature review focused on a research question that tries to identify, appraise, select and synthesize all high quality research evidence relevant to that question.
The evidence shows
Rita’s reply:
“However, what I do believe is that the burden of proving safety and effectiveness lies with the pro-fluoridation side”
“It also appears to me that the pro-fluoridation side is playing “whack a mole” with the studies weighing against CWF – often trying to hammer down/marginalize the opposition each time a negative study pops up, rather than trying to consider the evidence objectively.”
“However, to me, if even one strong study exists, then the entire compulsory practice must be re-evaluated.”
My Reply:
The scientific consensus is that fluoridation works, it is safe and it is cost effective. We have evolved with fluoride and had it adjusted in our water for over 60 years in some countries. Developed countries where natural fluoride levels are low but choose not to use community water fluoridation (CWF) generally use other methods such as milk and salt fluoridation, which again are both safe and effective, or have very effective public health and dental systems. Over 5,500 papers have been systematically reviewed and no consistent association between fluoridation and illness has been found that has been confirmed through later research.
Using the latest evidence: Public Health England just released their water fluoridation review this month – “Water fluoridation Health monitoring report for England 2014” and it concluded:
“This monitoring report provides evidence of lower dental caries rates in children living in fluoridated compared to non-fluoridated areas. Similarly, infant dental admission rates were substantially lower. There was no evidence of higher rates of the non-dental health indicators studied in fluoridated areas compared to non-fluoridated areas. Although the lower rates of kidney stones and bladder cancer found in fluoridated areas are of interest, the population-based, observational design of this report does not allow conclusions to be drawn regarding any causative or protective role of fluoride; similarly, the absence of any associations does not provide definitive evidence for a lack of a relationship.”
Last month a review “Health effects of water fluoridation: A review of the scientific evidence” written on behalf of the Royal Society of New Zealand and the Office of the NZ Prime Minister’s Chief Science Advisor concluded:
“Councils with established CWF schemes in New Zealand can be confident that their continuation does not pose risks to public health, and promotes improved oral health in their communities, reducing health inequalities and saving on lifetime dental care costs for their citizens. Councils where CWF is not currently undertaken can confidently consider this as an appropriate public health measure, particularly those where the prevalence and severity of dental caries is high. A forthcoming study from the Ministry of Health is expected to provide further advice on how large a community needs to be before CWF is cost-effective (current indications point to all communities of 1000+ people).
It is recommended that a review such as this one is repeated or updated every 10 years – or earlier if a large well-designed study is published that appears likely to have shifted the balance of health benefit vs health risk.”
Looking at the many other systematic reviews you will find a similar pattern. CWF is shown to be safe and effective. So the “burden of proof” really is on those claiming evidence of harm. They need to produce well supported and peer-reviewed studies which back up their claims.
If there is a strong evidence for health risks of fluoridation then I totally agree with Rita that it needs to be re-evaluated. Every year many studies are written on fluoridation and continued monitoring of the scientific findings occurs in many countries with the precautionary principle of being alert to any possible negative effects.
Health organisations
Rita’s reply:
“Please also note that any and all of your cites to the ADA lobby, or to the CDC (which, though its oral health division, works hand in hand with the ADA promoting fluoridation and thus has a serious conflict of interest/credibility problem) are unpersuasive to me – as they should be to anyone conducting even a minimum level of research into the history of and politics behind fluoridation (some of which is chronicled in my article, including the story of the EPA’s NTEU battle).”
“it does not take long to discover how politically motivated many “public health agencies” and “professional dental associations” are — or how willing they are to obscure, minimize, or bury contrary evidence or to marginalize the anti-fluoridation messengers, regardless of the evidence or the credentials of those messengers (e.g., Waldbott, Taylor, Marcus, Mullenix, Bassin, Hirzy).”
My reply:
I think Rita is placing her own bias on these judgments. One could equally say: “It does not take long to discover how politically motivated Dr Paul Connett and FAN are — or how willing they are to obscure, misinform, or bury contrary evidence or to marginalise the pro-science messengers, regardless of the evidence or the credentials of those messengers.”
If Rita has a specific problem with the CDC or the ADA, I can use some of the many other hundreds of health organisations around the world. They all have similar conclusions about fluoridation. As I said in my first response, there is not one reputable health organisation that is against fluoridation. We already have Dr Paul Connett suggesting a massive conspiracy, I hope you do not agree with his accusations as this is generally the last resort for people who cannot find reasonable faults in the evidence but still refuse to believe it.
NRC Report
Rita’s reply:
“However, I believe that its review of fluoride toxicology is highly relevant to exposures from fluoridated water (and its exposure data itself suggests that some people drinking fluoridated water can, indeed, receive doses that can cause adverse health effects, including severe dental fluorosis and bone fractures).”
“In addition, in a number of health risk areas, the NRC panel concluded that there was not enough data, and/or that more research needed to be conducted, before definitive statements could be made with respect to other potential adverse health effects due to excess exposure to fluoride.”
My reply:
I will not repeat what I said in my earlier reply. The review itself said that it was not relevant to exposures to concentrations used for fluoridated water and to say it is “highly relevant” is spreading misinformation. The NRC report furthered shows the safety of fluoridation. As for the “more research needed”, that is always the case with science. That is why responsible public health agencies continue to monitor research findings.
Ethics
Rita’s reply:
“I would genuinely be interested in knowing why you feel so strongly that imposing this practice on everyone is ethically justifiable.”
“Thus, I am very curious as to why there appears to be such an aggressive campaign on the pro fluoridation side to impose this practice on the world – and why anyone believes that personal liberties and rights to bodily integrity should be sacrificed for a public health practice addressing a non-contagious disease.”
“I would also be interested in understanding where you personally believe compulsory public health practices should begin and end (e.g., do you believe governments should mandate compulsory flu shots? What about the HPV vaccine that the Governor of Texas tried to mandate for girls? Where should the personal right to bodily integrity begin and end, in your opinion? And how comfortable are you with public health officials mandating what is good for you?…)”
My reply:
I don’t see how you conclude that I “feel so strongly that imposing this practice on everyone”. I, myself, could say I am strongly against misinformation. The MSoF society is here to help explain what the actual scientific evidence shows to the public, not to advocate for CWF at any cost. It is up to the communities if they want to use CWF and we, the MSoF Society, support their democratic right to decide.
But regarding ethical aspects, you might be interested in what the Nuffield Council on Bioethics decided. It:
- Rejected the prohibition of water fluoridation based on the argument of mass medication and restricting personal rights.
- Affirmed that water fluoridation should be accepted based on the quantified risks and benefits, the potential alternatives, and, where there are harms, the role of consent.
They also used a ‘stewardship mode’ to analyse the acceptable degree of state intervention to improve population health, concluding that water fluoridation can be justified based on its contribution to the goals of stewardship: the reduction of health inequalities, the reduction of ill health, and the concern for children, who represent a vulnerable group.
The New Zealand High court this year ruled that fluoridation of the water supply:
- is not a medical treatment,
- does not violate the right to refuse medicine,
- is not in breach of the Bill of Rights,
And that
- the Council was thoughtful and responsible in making their decision to begin fluoridation, and had no obligation to consider “controversial factual issues” (anti-fluoride propaganda).
You could say there is an aggressive campaign on both sides, but people are pushing for fluoridation simply because it works – reducing up to 40% of caries over a whole population.
Dental caries is a serious chronic disease, it makes no difference if it is contagious or not. The Royal Society Review pointed out that
“…tooth decay (dental caries) remains the single most common chronic disease among New Zealanders of all ages, with consequences including pain, infection, impaired chewing ability, tooth loss, compromised appearance, and absence from work or school. Tooth decay is an irreversible disease; if untreated it is cumulative through the lifespan, such that individuals who are adversely affected early in life tend to have pervasive decay by adulthood, and are likely to suffer extensive tooth loss later in life. Prevention of tooth decay is essential from very early childhood through to old age”.
The Royal Society Review also suggested that removing fluoridation would have direct and indirect costs to society.
“Tooth decay is responsible for significant health loss (lost years of healthy life) in New Zealand. The ‘burden’ of the disease – its ‘cost’ in terms of lost years of healthy life – is equivalent to 3/4 that of prostate cancer, and 2/5 that of breast cancer in New Zealand. Tooth decay thus has substantial direct and indirect costs to society.”
I am all for protecting the vulnerable. If individuals do not consent, they can simply choose not to partake of the community water supply (bottled water, filters, rain water, etc.). I feel this is starting to head slightly off-topic but to answer your question, if the vaccine given out is safe and effective for the general public then I have no problems with compulsory shots for children. While choice is nice thing to have, you cannot always get it, especially if it is going to lower the quality of life in children.
The New Zealand High court summarised some ethical aspects in the decision I referred to above:
“Provided it does not have consequences for public health a person has the right to make even the poorest decisions in respect of their own health. But where the state, either directly or through local government, employs public health interventions, the right is not engaged. Were it otherwise, the individual’s right to refuse would become the individual’s right to decide outcomes for others. It would give any person a right of veto over public health measures which it is not only the right but often the responsibility of local authorities to deliver.”
The World Health Organization
Rita’s reply:
“Data published by the WHO suggests that the decline in dental caries is similar in both fluoridated and unfluoridated countries, and I have heard of no massive outbreak of a worldwide dental carie epidemic that has been attributed to a lack of fluoridated water (rather than to poverty, poor nutrition, or a lack of access to proper dental care).”
My reply:
Petersen & Lennon (2004), a WHO funded study showed dental caries remain a major public health concern, affecting 60–90% of schoolchildren and the vast majority of adults. While fluoride is not a silver bullet, it is just part of the problem, it should not be ignored when it can clearly help very effectively. Their study goes into a number of suggestions for alleviating tooth decay, one being fluoridation.
“Water fluoridation, where technically feasible and culturally acceptable, has substantial advantages particularly for subgroups at high risk of caries. Alternatively, fluoridated salt, which retains consumer choice, can also be recommended. WHO is currently in the process of developing guidelines for milk fluoridation programs, based on experiences from community trials carried out in both developed and developing countries.”
As for the similar DMFT decline between fluoridated and unfluoridated countries Rita claims this needs to be considered critically. Fluoride occurs naturally everywhere and it is very hard to compare one country to others because of the many other contributing factors such as; history, culture, ethnic differences, as well as differences in health services, dental practice and assessments. 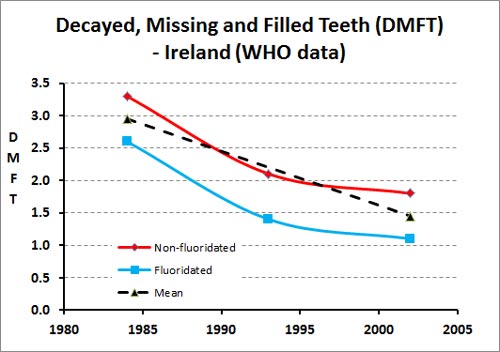 The graphical evidence FAN promotes on their website and elsewhere they do not account for naturally occurring fluoride or other programs (fluoride vanish, mouth rinse programs, etc.) and different history and social practices. Their graphs also use only 2 data points for each country. There is no consideration of also changing fluoridation amounts over time and their graph is very confusing. It does not enable proper consideration of different DMFT declines in different countries. The stats show Denmark having the lowest DMFT and FAN marked them as not fluoridated, but they actually have high levels of naturally occurring fluoride.
The graphical evidence FAN promotes on their website and elsewhere they do not account for naturally occurring fluoride or other programs (fluoride vanish, mouth rinse programs, etc.) and different history and social practices. Their graphs also use only 2 data points for each country. There is no consideration of also changing fluoridation amounts over time and their graph is very confusing. It does not enable proper consideration of different DMFT declines in different countries. The stats show Denmark having the lowest DMFT and FAN marked them as not fluoridated, but they actually have high levels of naturally occurring fluoride.
If you look at the WHO data in more detail (graph left does this for the Irish Republic using the same WHO data) you will find that fluoridated areas show faster declines in DMFT than unfluoridated areas.
Making Sense of Fluoride
Rita’s reply:
“…you complain about FAN not being a legitimate source of credible scientific information, but your organization is also a political advocacy (pro-fluoridation) group”
“I urge you to conduct such a battle with a more appropriate sparring partner, such as FAN-NZ.”
My reply:
Like yourself, I am not a scientist – I am a software developer; my responses get checked by scientists but I would always look into the evidence in scientific studies. I avoid political or activist organisations (legitimate or not). The Making Sense of Fluoride society is not a pro-fluoridation group, we are a pro-science group. We will go with what the scientific consensus says and will spread warnings, if for example: sometime in the future, CWF was really found to be harmful.
The objectives of the MSoF incorporated society are:
- To foster awareness and dispel misinformation regarding fluoride with a focus on CWF.
- Use the scientific method as the foundational platform upon which this awareness is promoted.
FANNZ, now known as Fluoride Free NZ (and a close partner of FAN), will always be anti-fluoride no matter what the evidence shows. For that reason it is usually not fruitful debating them. Their incorporated society main purposes make clear their opposition to CWF irrespective of the science:
- To bring about the permanent end to public water fluoridation (“fluoridation”) in New Zealand.
- To provide resources, both personal and material, to others opposing fluoridation in New Zealand.
- To provide a central contact point for those opposing fluoridation in New Zealand.
Apology
Rita’s reply:
“This statement about “mounting scientific evidence” at the start of my paper (near fn. 2) actually references an entire section of my article – (“See discussion infra Sec. II-B”) — and not an opinion piece by Colquhoun, which is only referenced – appropriately – at footnote 65 (referring to “formerly avid fluoride proponents” who have changed their minds). I have no desire to engage with insincere zealots, so I hope that you simply made a mistake there.”
My reply:
I apologise for mistaking you and any offense it may have caused you. It was clearly a simple mistake that anyone could have made and I had no intention to twist your words.
Wrapping up
Rita’s reply:
“After this exchange, however, I am only interested in a private discussion with you, which is something you may not be interested in as it may not advance your organization’s agenda”
“However, your Facebook posting has generated some contact to me by a few rude (and seemingly unbalanced) pro fluoridation folks”
My reply:
MSoF is always happy to have private discussions if you are willing to listen to our feedback. A lot of our work is outside of what the public sees but we always up for public exchanges to share to our followers.
You will find that your paper got sent all over Facebook and the media; because it was publicised in a press release from FAN. That is how I found out about it. It is a pity you were subjected to insults because of that publicity. That said I was also hit with insults on Fluoride Free NZ Facebook pages because of my response to you. These insults are common and something I have gotten used too; in either case it is a shame that people feel it best to engage in debate in disrespectful ways. Fluoridation is an emotional topic for some – personally I do my best to stick with the science and keep my emotions out.
Thank you Rita for making time in reading our feedback and responding to us.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
I came here to look for a reference to a systematic review of studies on cancer site in the body, male vs female, and fluoride levels at those appropriate to fluoridation. Typing in “systematic” brought me to this article.
Have a read of my first reply:
http://msof.nz/2014/09/compulsory-water-fluoridation-a-response-to-rita-barnett-rose-discussion/
Or you might be interested in:
http://msof.nz/2014/02/a-look-into-osteosarcoma/