I have contacted Associate Professor Rita Barnett-Rose about her unpublished paper “Compulsory water fluoridation: justifiable public health benefit or human experimental research without informed consent” (you can read a copy here: http://works.bepress.com/rita_barnett/3/).
It concluded that “The evidence continues to suggest that compulsory water fluoridation is no longer justifiable as a public health benefit” and “human rights burden and economic costs are not reasonable or justifiable”.
There were claims about the science which (presumably) are important for the legal/ethical conclusions. We at Making Sense of Fluoride felt there was misinformation on the science and a public exchange would be a good way to engage in a discussion of the claims – even withdrawing those claims if found wrong. We thank Rita for listening to us and hope that we find common ground even if it’s just in the science.
Feel free to comment on any side of the discussion.
You can grab the PDF version here.
Compulsory Water fluoridation: A Response to Rita Barnett-Rose
Written by Daniel Ryan
Introduction
I have contacted Associate Professor Rita Barnett-Rose about her unpublished paper “Compulsory water fluoridation: justifiable public health benefit or human experimental research without informed consent” (you can read a copy here: http://works.bepress.com/rita_barnett/3/). It concluded that “The evidence continues to suggest that compulsory water fluoridation is no longer justifiable as a public health benefit” and “human rights burden and economic costs are not reasonable or justifiable”.
There were claims about the science which (presumably) are important for the legal/ethical conclusions. We at Making Sense of Fluoride (MSoF) felt there was misinformation on the science and a public exchange would be a good way to engage in a discussion of the claims – even withdrawing those claims if found wrong. We thank Rita for listening to us and hope that we find common ground even if it’s just in the science.
Discussion
For the most part of this discussion I will stick to pages 13-19 with the header “Scientific Evidence against Compulsory Water Fluoridation” and breaking down into the sub-headers.
First off, looking at the sources used, there are many that are comments and articles from political activists rather than primary research sources. For example Fluoride Action Network is not a credible scientific organisation. This is not a good way of reviewing the scientific literature; in fact it is very poor practice. This is a fundamental problem with this paper.
The paper starts off saying there is mounting scientific evidence against fluoridation. The evidence used was an opinion piece from John Colquhoun. Dental Watch has a paper “Why We Have Not Changed Our Minds about the Safety and Efficacy of Water Fluoridation: A Response to John Colquhoun” that critiques his paper.
“His paper rehashed earlier criticisms of water fluoridation, using selective and highly biased citations of the scientific and non-scientific literature”.
“Why I Am Now Officially Opposed to Adding Fluoride to Drinking Water” from Dr. Hardy Limeback and “Dr. William Hirzy Portland letter” are also opinion pieces. It is important to note that Dr. Hardy Limeback is a member of the Advisory Board of Paul Connett’s Fluoride Alert Network. Dr. William Hirzy works for Fluoride Action Network as a paid political lobbyist. “Mounting scientific evidence”- nothing could be further from the truth. There is not one reputable health organisation that is against fluoridation.
1: Dental Fluorosis
There is no argument that having too much fluoride when the teeth are forming will cause dental fluorosis but this isn’t the case for fluoridation. There is little difference in frequency and severity of fluorosis between non-fluoridated and fluoridated areas, something which Barnett-Rose (2014) seems to ignore. The CDC source given was looking at fluorosis as a whole and not at fluoridated vs non-fluoridated, but it states that:
“community water fluoridation programs were developed to add fluoride to drinking water to reach an optimal level for preventing tooth decay, while limiting the chance of developing dental fluorosis”.
If there were any large differences in fluorosis then I would be all for another look into balancing the levels of fluoride in those areas. In fact health authorities in many countries continually monitor research findings for this very reason and that was the reason for the National Research Council (2006) review which did recommend reducing the primary MCL of 4 ppm.
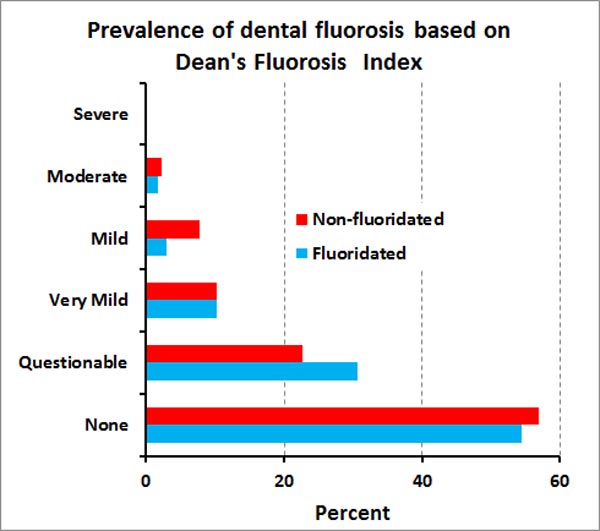
Any increase in fluorosis due to CWF would be in the very mild to mild fluorosis range. The dental fluorosis about which they speak in Warren’s et al. (2009) “Iowa study” is overwhelmingly of the barely detectable nature. The 2009 New Zealand Oral health Survey found very little difference between fluoridated and non-fluoridated areas, in terms of the levels of mild to very mild fluorosis (which has no effect on appearance, form or function of teeth), as shown on the graph below. In fact, Lida & Kumar (2009) have demonstrated mildly fluorosed teeth to be more decay resistant.
The statement that fluorosis is “the first sign of fluoride toxicity” is debatable. What sign of which particular toxicity? Just because there might be other effects which have not yet been shown is not proof that there are other effects. It presumably has been a common feature of teeth through the centuries and is harmless.
The American Dental Association website says,
“Yes, it is safe to use fluoridated water to mix infant formula. If your baby is primarily fed infant formula, using fluoridated water might increase the chance for mild enamel fluorosis, but enamel fluorosis does not affect the health of your child or the health of your child’s teeth”.
The recommendation by health authorities that parents use unfluoridated water to make up formula is a peace-of-mind suggestion, not a firm recommendation. For example the CDC says:
“However, if your child is exclusively consuming infant formula reconstituted with fluoridated water, there may be an increased chance for mild dental fluorosis. To lessen this chance, parents can use low-fluoride bottled water some of the time to mix infant formula”.
For infants and children in their tooth-developing years of 0-8, the upper limit (UL) for fluoride is lower, but only due to a risk of development of mild dental fluorosis. That’s why the UL for daily fluoride jumps to 10mg/day after age 8, once the teeth are formed.
The rest of the “Dental Fluorosis” section in Barnett-Rose (2014) talks about moderate to severe dental fluorosis, which is not caused by community water fluoridation and so is pointless to discuss.
2: Skeletal Fluorosis and Bone Fractures
Again, there is no disagreement that chronic exposure to high levels of fluoride can cause skeletal fluorosis and increase the risk of bone fractures. But you don’t see these problems at levels of 0.7-1.2 ppm in community drinking water. The Institute of Medicine has established that the daily upper limit for fluoride intake from all sources, for adults, before adverse effects will occur, short or long-term, is 10 mg. There is no quality research to show skeletal fluorosis can develop at the levels of 0.7-1.2ppm. Even the source used in Barnett-Rose (2014) says “Crippling skeletal fluorosis may be produced by levels of 10-20 mg/day over 10-20 years”.
National Fluoridation Information Service has released a report this month on fluorosis and concluded:
“There are no known health risks associated with CWF in New Zealand, and no severe dental fluorosis, or skeletal fluorosis, has been found. While fluoride is incorporated into teeth and bones, there is no robust evidence of toxic accumulation of fluoride in other tissues in the body”.
It also noted in its conclusion:
“As with many vitamins and minerals, such as iron, and vitamins A and D, fluoride intakes at high levels can be toxic. However, it is impossible to experience acute fluoride toxicity from drinking water optimally fluoridated at levels between 0.7 mg/L to 1.0 mg/L (MoH, 2009), and there is no evidence of skeletal fluorosis resulting from CWF in New Zealand. It makes sound clinical sense to ingest a substance at a level that achieves maximum benefit with minimal adverse effects (Bowen, 2002)”.
One needs to be careful of cherry picking scientific studies. When you look at all the data you will find bone fracture is not an issue. Vestergaard et al. (2007), in a meta-analysis that used 25 studies, came to the conclusion that
“there was no effect on hip or spine fracture risk”. He also noted that “in subgroup analyses a low fluoride dose (< or =20 mg/day of fluoride equivalents) was associated with a significant reduction in fracture risk”.
This showed that fluoridation can help bones when at the optimum fluoride levels.
Ingestion of some fluoride is necessary as the bioapatites in our body contain both fluoride and carbonate as normal, natural components. The incorporation of ions like fluoride into bioapatites can change their solubility product by several orders of magnitude according to Driessens (1973). Posner et al. (1963) attribute the improved stability of bone to “the isomorphous substitution of fluoride in the apatite structure”.
3. Pineal Gland and Endocrine Disruption Studies
Fluoride can accumulate in the pineal gland. Calcification of the pineal gland is caused by calcium, phosphate and old age. Because the bioapatites in calcified tissues are actively undergoing mineralisation and remineralisation they easily incorporate fluoride into their structure and this leads to higher concentration of fluoride in calcified tissues than in bones generally. No evidence of harm has been found.
There is no known link to hypothyroidism at the levels we get in water fluoridation. I’m not sure where the evidence for “The fluoride dose capable of reducing thyroid function is low – just 2 to 5 mg per day over several months” from Barnett-Rosie (2014). Her source, the Fluoride Action Network website, points to a study Galletti & Joyet (1958), which says
“Our aim was to elucidate the inhibitory effect of chronic administration of fluoride upon thyroid function in cases of hyperthyroidism. It was demonstrated that such an action appears only occasionally among persons subjected to massive doses of this substance”.
The study was working with prolonged administration of a daily dose of 2-20 mg (on top of their diet). This was also a very small study of 15 people who suffered from hyperthyroidism. Galletti also noted that
“Despite the relatively large amounts administered (up to 20 mg. of F~ for one injection), neither immediate nor delayed toxic manifestations were observed”.
This demonstrates my point that primary sources should be used, and definitely not activist websites.
The ADA concludes on its fluoridation facts document,
“There is no scientific basis that shows fluoridated water has an adverse effect on the thyroid gland or its function”.
It also states:
“The researchers concluded that prolonged ingestion of fluoride at levels above optimal to prevent dental decay had no effect on thyroid gland size or function. This conclusion was consistent with earlier animal studies”
4. Cancer Studies
Bassin (2006) data presentation did not show how many cases and controls were included in each of the models; and fluoride exposures were estimated rather than measured directly. The authors commented that “Further research is required to confirm or refute this observation”.
The NHMRC (2007) observed that:
“Shortcomings in their study mean the results should be interpreted with caution pending publication of the larger study results. Co-investigators of Bassin point out that they have not been able to replicate these findings in the broader Harvard study that included prospective cases from the same 11 hospitals”.
There is no demonstrable link between fluoride and cancer. The American Cancer Society says:
“The general consensus among the reviews done to date is that there is no strong evidence of a link between water fluoridation and cancer”.
The National Cancer Institute says
“Fluoride in water helps to prevent and can even reverse tooth decay. More than 60 percent of the U.S. population has access to fluoridated water through public water supply systems. Many studies, in both humans and animals, have shown no association between fluoridated water and cancer risk”.
This is backed up by systematic reviews e.g. the York Review (2000) reported:
“No clear association between water fluoridation and osteosarcoma”.
National Research Council (2006) commented,
“Assessing fluoride as a risk factor for osteosarcoma is complicated by the rarity of the disease and that population is all generally exposed to some level of fluoride”.
SCHER (2010) reported:
“a possible link between fluoride in drinking water and osteosarcoma, but studies are equivocal. No evidence from animal studies to support the link, and thus fluoride cannot be classified as to its carcinogenicity”.
5. Lower IQ’s in Children
It is debatable that Mullenix et al. (1995) interpretation on the study was flawed, it doesn’t matter if it was in a “well-respected peer reviewed journal” or not. Plenty of well-respected journals have released poor papers. One such example was Wakefield’s (1998) claim of a link between vaccines and autism, published in The Lancet.
The study by Mullenix et al. (1995) was refuted by Ross & Daston (1995):
“In summary, much of the ambiguity in the interpretation of these results could have been avoided with information from two concurrent or historical control groups: 1) a group to define the behavioral signature resulting from long term adulteration of the drinking water, and 2) a group to define the behavioral signature of animals with hippocampal damage in this testing system. Such controls are an essential feature of test validation and experimental design. Novel behavioral chemicals of unknown toxicity are dosed, and all possible results interpreted as neurotoxicity. Instead, both positive and negative control materials should be evaluated, and the results linked with well-characterized functional and morphological indices of neurotoxicity.
We appreciate the opportunity to provide our interpretations of this study. We do not believe that the study by Mullenix et al. can be interpreted in any way as indicating the potential for NaF to be a neurotoxicant”
On top of that, it is also debatable if plasma levels in rodents due to high levels of fluoride are equivalent to those in humans. The National Research Council (2006) discussed the contradictory data used for attempting to show a ratio between humans and rats for blood plasma levels and concluded:
“Dunipace et al. (1995) concluded that rats require about five times greater water concentrations than humans to reach the same plasma concentration. That factor appears uncertain, in part because the ratio can change with age or length of exposure. In addition, this approach compares water concentrations, not dose. Plasma levels can also vary considerably both between people and in the same person over time (Ekstrand 1978)”.
Choi (2012) described 27 studies found majority in obscure Chinese scientific journals. China is not artificially fluoridated and the studies used high levels of naturally occurring fluoride in the well water of various Chinese, Mongolian, and Iranian villages. The concentration of fluoride in these studies was as high as 11.5 ppm. By the admission of the Harvard researchers, these studies had key information missing, used questionable methodologies, and had inadequate controls for confounding factors. These studies were so seriously flawed that the lead researchers, Anna Choi, and Philippe Grandjean, were led to issue a statement in September of 2012. Anna Choi said:
“These results do not allow us to make any judgment regarding possible levels of risk at levels of exposure typical for water fluoridation in the U.S. On the other hand, neither can it be concluded that no risk is present“.
Broadbent et al. (2014) used data from the Dunedin Multidisciplinary Study, which is world-renowned for the quality of its data and rigour of its analysis, and found no significant differences in IQ by fluoride exposure, even before controlling for the other factors that might influence scores. It controlled for childhood factors associated with IQ variation, such as socio-economic status of parents, birth weight and breastfeeding, and secondary and tertiary educational achievement.
6: Benefits from Systemic Fluoride Intake?
For this section I’ll limit the discussion to the benefits of systemic and topical intake of fluoride.
Even if the primary role of fluoride was topical, water fluoridation has a beneficial effect and makes a good delivery system. Consumption of fluoridated food and water enables transfer of fluoride to saliva and biofilms on the teeth. This fluoride, together with calcium and phosphate on the saliva, reduces acid attack on the teeth and so helps prevent tooth decay. Because fluoride concentrations in saliva decrease within an hour or so after brushing, fluoridated water complements use of fluoridated toothpaste. Our teeth are in more regular contact with food and water than they are with toothpaste.
Buzalaf et al. (2011) reports:
“More than 60 years of intensive research attest to the safety and effectiveness of this measure to control caries. In this case, however, it should be emphasized that despite being classified as a ‘systemic’ method of fluoride delivery (as it involves ingestion of fluoride), the mechanism of action of fluoridated water to control caries is mainly through its topical contact with the teeth while in the oral cavity or when redistributed to the oral environment by means of saliva. Since fluoridated water is consumed many times a day, the high frequency of contact of fluoride present in the water with the tooth structure or intraoral fluoride reservoirs helps to explain why water fluoridation is so effective in controlling caries, despite having fluoride concentrations much lower than fluoride toothpaste, for example. This general concept can be applied to all methods of fluoride use traditionally classified as ‘systemic’. In the light of the current knowledge regarding the mechanisms by which fluoride control caries, this system of classification is in fact misleading”.
Featherstone (2000) also demonstrated that:
“The cariostatic effects of fluoride are, in part, related to the sustained presence of low concentrations of ionic fluoride in the oral environment, derived from foods and beverages, drinking water and fluoride-containing dental products such as toothpaste. Prolonged and slightly elevated low concentrations of fluoride in the saliva and plaque fluid decrease the rate of enamel demineralization and enhance the rate of remineralization”.
The main benefit is from topical application but systemic ingestion still plays a role. Buzalaf et al. (2011) also states that:
“Evidence also supports fluoride’s systemic mechanism of caries inhibition in pit and fissure surfaces of permanent first molars when it is incorporated into these teeth pre-eruptively”.
Quality studies continue to show fluoridation to be effective today. Newbrun (1989), Brunelle & Carlos (1990) and Griffin et al. (2007) have proven water fluoridation continues to be effective in reducing dental decay by 20-40%.
National Research Council Report
I will touch on the National Research Council (2006) report as Rita has asked me to give my assessment and it is used throughout her paper. The 2006 NRC Committee was charged with evaluating the adequacy of the US EPA primary (4 ppm) and secondary (2 ppm) MCLs for fluoride to protect the public against adverse effects, it did not look at the benefits. The EPA’s guidelines are not recommendations about adding fluoride to drinking water to protect the public from dental caries. Guidelines for that purpose (0.7 – 1.2ppm) were established by the U.S. Public Health Service. It reported:
“this report does not evaluate nor make judgments about the benefits, safety, or efficacy of artificial water fluoridation. That practice is reviewed only in terms of being a source of exposure to fluoride”.
After the Committee looked at all relevant fluoride literature, it recommended that the EPA primary MCL for fluoride be lowered from 4.0 ppm. The stated reasons for this recommendation were the risk of severe dental fluorosis and bone fracture with chronic ingestion of water with a fluoride content of 4.0 ppm or greater. No other reasons. Had this Committee had any other concerns with fluoride at this level, it would have stated so and recommended accordingly. Additionally, this Committee made no recommendation to lower the EPA secondary MCL for fluoride, 2.0 ppm which water fluoridation at 0.7ppm is 1/3 of this value.
In March of 2013, Dr. John Doull, the internationally respected toxicologist who chaired the NRC committee, made the following statement:
“I do not believe there is any valid, scientific reason for fearing adverse health conditions from the consumption of water fluoridated at the optimal level.”
Final recommendation of this Committee showed nothing that doubt on the safety of fluoride at the recommended optimal level. It also has no bearing on water fluoridation so using the NRC report to as a reason to stop fluoridation would be misguided.
Conclusion
I have outlined major flaws of the science of this paper, with the major criticism being not using primary sources. There was no assessment of the quality of the evidence. One should start with secondary reviews published in peer-reviewed, high-impact journals, including meta-reviews, review articles, and Cochrane Collaboration reviews; otherwise, high quality clinical trial reports with fairly large number of subjects.
Any further discussions on the ethics or legal matters with fundamental flaws in the science would make any exchange confusing and pointless.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
[…] original paper here. My first response here. Rita’s first response […]
[…] You can read Part 1 of the public exchange here. […]
[…] My first response […]